Where is the tibia. Anatomy and possible damage to the tibia and fibula. Where is the fibula located
The article will focus on the fibula, where it is located, injuries and fractures, description + Photo, read in detail below in the article \u003e\u003e
Man is the most complex mechanism in its structure. It contains a lot of bones, cells, tissues, etc. The human limb is composed of long and short muscles, tendons, bones, nerve fibers, and other tissues.
All of them interact with each other, creating the ability to move. Many people know what a shin is.
Fibula. General information
Place in the human body
The lower leg consists of the tibia and fibula. The fibula looks like an elongated tube and is the smaller bone of the lower leg.
She has her own body and two peaks. The lower part is called the lateral ankle and takes part in the formation of the ankle joint. It is a kind of joint stabilizer.
The fibula is hardly stressed while walking. Its main function is to participate in the formation of the ankle and knee joints. In appearance, the bones of the legs seem to be more massive than, for example, arms, but despite this, they are often injured.
Damage to the fibula often affects the tibia, causing displacement complications and osteomyelitis. In case of fracture of only a small bone, recovery is faster and more efficient.
From anatomy
In the musculoskeletal system of an adult, there are passive and active parts.
Active - these are muscles and ligaments.
Passive - bones and their joints.
The adult skeleton consists of 208 bones. In order to distribute body weight correctly, the bones are hollow inside. Due to which the weight of all bones is less in contrast to the weight of the body. But, nevertheless, bones are strong and able to withstand adequate loads.
The structure of the fibula
If you disassemble the topography, then the small bone is located between the thigh and the foot at the bottom of the leg. Above, it borders on the knee, and below on the ankle.
Divided into 3 parts.
Body or diaphysis
How to identify a fibular fracture
With this nature of the injury, the picture is typical. A person faces:

In this case, factors conducive to injury are as follows:
- - deficiency of vitamin D, calcium;
- - elderly age;
- - fragility of bones in early childhood;
- - pathologies affecting the state of the bones;
- - strong blow.
Childhood fractures
Often, children under the age of three will break the fibula. This happens for several reasons, and one of them is a fall from a height. These fractures are rarely open.
Symptoms - painful response to touch, problem with raising the leg, swelling of soft tissues.
At this age, X-rays are not always a good solution, so bone scanning is more often used for diagnosis. If the fracture is confirmed, therapy begins. A short bandage with a cast is applied to the leg until the leg is restored.
Full rehabilitation usually occurs more quickly than in the case of adult patients. The reason is the accelerated metabolism.
Sports-related fractures
The result of treatment directly depends on the patient's compliance with the doctor's recommendations. It is very important to protect the injured limb from physical exertion during the rehabilitation period and after.
Important! The treatment outcome is influenced by the time of seeking help - the earlier, the higher the chance of successful therapy and recovery.
Consequences after treatment
After traditional or surgical intervention, you may experience:
- dysfunction in the ankle;
- constant swelling at the site of injury;
- deforming arthrosis;
- osteochondrosis;
- dependence on natural conditions.
Take care of your feet! When cycling, rollerblading, skating, use shin guards, knee pads, etc.
Bone strength depends on the amount of calcium in the body. A healthy lifestyle and caution can protect against many injuries.
In situations with a fracture of the fibula, a person should not despair and urgently receive qualified medical care. After an injury, try to protect your legs from re-injury throughout your life.

The fibula is represented by an elongated tubular formation. The bone is represented by the body, or diaphysis, and two vertices, called the epiphyses. The lower fragment, called the lateral ankle, is involved in the creation of the ankle joint. The lateral ankle acts as a kind of stabilizing factor in the joint located between the lower leg and foot.
Anatomy and position relative to other bones
The musculoskeletal system (MSA) in adults is represented by active and passive parts. The active component includes muscles, ligamentous apparatus. A passive fragment is indicated by a skeleton consisting of bones and their joints. In the body of an adult, this part is represented by 208 bones. In order to properly redistribute a person's body weight in the process of life, the inner part of the bones is hollow. With the help of this, the weight of the skeleton is less in comparison with the total mass, however, despite this, the structure of the bones is strong, which allows the body to function adequately to the supplied loads.
To appreciate the physiological significance of the tibia, it is necessary to understand their topography. The fibula is located in the lower part of the skeleton (leg area), between the thigh and the foot, in contact with the tibia. Above, the shin bones are limited by the knee joint, from below by the ankle. The small bone is connected to the foot through the lateral ankle through the ankle joint. Large ligaments are located between the tibia.
In accordance with the length in the tibia, 3 parts are distinguished: the diaphysis (body) and 2 pineal glands (upper, lower fragment). The body of the bone is bent backwards and twisted along the axial direction. The diaphysis is represented by a prism and consists of three faces: medial, lateral and posterior. Each of the edges is separated by a ridge. The medial and lateral edges are separated by the anterior protrusion, the inner (medial protuberance) divides the medial and posterior sides of the bone, the posterior ridge is located between the posterior and lateral sides.
On the back of the MBC there is an opening for the exit of blood vessels and nerves. From this hole, a special channel extends distally into the bone, communicating with the channels of other areas of the skeleton through holes. On the inner side between the bones there is a demarcation edge. The upper epiphysis, represented by the head, contacts the tibia with the articular side. The top is pointed. The head is connected to the shaft of the fibula through the neck.
One of the most important formations of the fibula is distinguished by the peculiarity of topography and interaction with the bones of the foot and lower leg through the lower pineal gland. The distal portion of the bone is often referred to as the lateral malleolus. This ankle can be easily palpated through the skin when the foot is flexed forward.
 On the inner side of the lower epiphysis, the articular side is located, providing the connection between the talus and the lateral malleolus. Slightly higher in the fibula, there is a slight roughness that connects with the peroneal notch in the tibia. There is an ankle groove on the back of the fibula. The peroneal tendon passes through this depression.
On the inner side of the lower epiphysis, the articular side is located, providing the connection between the talus and the lateral malleolus. Slightly higher in the fibula, there is a slight roughness that connects with the peroneal notch in the tibia. There is an ankle groove on the back of the fibula. The peroneal tendon passes through this depression.
Impact on functions in the musculoskeletal system
The leading function performed by the fibula, which is laid down in the process of ontogenesis, is the provision of rotation in the ankle. Rotation in this case is a turn to the right or left of the lower leg and foot in relation to each other. Given the anatomical structure, location, under the influence of a strong traumatic aspect, the bone tissue is prone to fractures.
Usually, the fracture appears for the first time in the tibia because it takes on the leading stress while walking. Massive injuries or strong local effects of a negative factor can cause damage to the tibia, often with rupture of soft tissues, and displacement of bone fragments. Fractures appear in various parts of the fibula. Most often noted in the lower pineal gland.
Tibia fracture options:

Fractures are usually combined with subluxation and dislocation of the foot, rupture of the distal syndesmosis between the tibia, and shortening of the bone. To understand that a fracture of the entire or a fragment of the fibula has occurred, it is necessary to note a number of characteristic symptoms, the main of which are pain at the site of the lesion, which increases with palpation and movements in the ankle or the application of a vertical load, edema.
The pain is noted constantly and intensifies when walking or standing. These symptoms usually occur after a leg injury or fracture. To restore bone function to the full, it is necessary to consult a traumatologist as soon as possible.
Briefly about therapeutic measures and healing times
Treatment of fibula fractures is carried out conservatively or surgically. First, they begin non-operative intervention. The conservative technique is based on the comparison of separated fragments of bone tissue and their subsequent retention. The primary point in the tactics of treatment, the traumatologist must carry out the reposition of the fragments, thereby excluding the further deployment of the MBC and subluxation or dislocation of the foot. If the reduction is successful, confirmed by the results of an X-ray examination, the ankle is closed with a plaster mass or orthosis.
In a situation where the docking and fixation of the bone pieces did not give the necessary results, a surgical intervention is prescribed, represented by a number of stages:

After the performed surgical intervention, the patient must undergo a rehabilitation period. The timing of the fusion of the fibula is individual, and in uncomplicated variants correspond to 2-3 months. When multiple bone fractures were noted, as well as a history of burdening (somatic pathology in the stage of compensation and decompensation), the fracture in the tibia continues to heal for six months. In order to accelerate the overgrowing of the fracture, to recreate the functions, the patient is prescribed therapeutic exercises and massage. Not in the acute period, treatment is supplemented with physiotherapy intervention.
Most people who are faced with fractures of the bones of the lower extremities, especially the tibia, which plays an important role in the development of the ankle joint, are worried about the further consequences and forecasts of qualified specialists.
The result of treatment depends not only on the correct comparison and fixation of the fragments. It is extremely important for the patient to strictly follow all the doctor's recommendations. It is especially necessary to protect the fracture area from unnecessary physical activity during the rehabilitation period and after. The earlier from the moment of the leg injury the patient seeks qualified help, the more likely it is for successful treatment and complete rehabilitation.
Sometimes after bone fracture, conservative or surgical interventions, the following consequences may occur:

To prevent movement problems after a bone or ankle fracture, it is necessary to take care of your legs. If an injury does occur, it is necessary to urgently consult a traumatologist.
After a fracture, the site of the lesion should be protected throughout life and not subjected to further physical exertion.
The skeleton of the free part of the lower limb (pars libera membrae inferioris) is made up of the femur, patella, shin bones and foot bones.
The femur (os femoris) (Fig. 55, 56), like the humerus, ulna and radius, is a long tubular bone, the proximal epiphysis of which ends with a head, and the expanded distal one has two condyles (medial and lateral). The diaphysis of the femur is slightly curved forward; its anterior surface is smooth, and along the posterior one there is a longitudinal rough line (linea aspera) (Fig. 46), in which the medial (labium mediale) and lateral (labium laterale) lips are distinguished (Fig. 46). Slightly below the upper epiphysis is a protrusion called the gluteal tuberosity (tuberositas glutea) (Fig. 46).
The head (caput ossis femoris) (Fig. 46) of the proximal epiphysis of the femur is connected to the diaphysis by a long neck of the femur (collum ossis femoris) (Fig. 46), somewhat compressed in the anteroposterior direction and forming an obtuse angle with the body of the bone (in men, this angle much more than women). In the center of the femoral head is the fossa of the femoral head (fovea capitis ossis femoris) (Fig. 46). The protrusions of the bone, located above and below in the place of transition of the bone body to the neck, - large (trochanter major) (Fig. 46) and small trochanter minor (Fig. 46) - are connected to each other by an intertrochanteric crest (crista intertrochanterica) ( Fig. 46) and the intertrochanteric line (linea intertrochanterica) (Fig. 46). The depression located at the base of the greater trochanter is called the trochanteric fossa (fossa trochanterica) (Fig. 46).
The medial (condylus medialis) and lateral (condylus lateralis) condyles (Fig. 46), located on the lower epiphysis of the femur, are separated from the back by the fossa intercondylaris (Fig. 46). In front, the condyles are closed, forming a platform for connection with the patella. In the formation of the knee joint, the posterior and lower surfaces of the condyles covered with cartilage are involved; each condyle corresponds to the epicondylus located above it (Fig. 46).
The patella, or patella (Fig. 54, 55, 56), which protects the knee joint in front, is fixed in the tendon of the quadriceps femoris muscle. The patella is a sesamoid bone in the shape of a triangle pointing downwards with a rough anterior surface. The smooth posterior surface is covered with articular cartilage.
The tibia of the lower leg (tibia) (Fig. 55, 56) is a long tubular bone with a massive (compared to the fibula) trihedral diaphysis, which, closer to the distal epiphysis, passes into a tetrahedron. The wide upper epiphysis of the bone ends in the medial (condylus medialis) and lateral (condylus lateralis) condyles (Fig. 49), the flat upper articular surface (facies articularis superior) (Fig. 47, 49) of which, covered with articular cartilage, is slightly concave and has a the center of the intercondylar eminence (eminentia intercondylaris) (Fig. 47, 49). The lateral condyle has another articular surface - the peroneal, located on its lateral surface and participating in the formation of the tibiofibular joint with the proximal epiphysis of the fibula.
| Figure: 46. Femur A - front view; B - rear view; B - left view (from the medial side): 1 - fossa of the femoral head; 2 - the head of the femur; 3 - large spit; 4 - the neck of the femur; 5 - intertrochanteric line; 6 - small spit; 7 - the body of the femur; 8 - lateral condyle; 9 - medial condyle; 10 - trochanteric fossa; 11 - intertrochanteric ridge; 12 - gluteal tuberosity; 13 - medial lip; 14 - lateral lip; 15 - rough line; 16 - medial epicondyle; 17 - lateral epicondyle; 18 - intercondylar fossa |
|
 |
|
 |
The medial, lateral and posterior surfaces (Fig. 47, 49) of the body of the tibia are separated by sharp edges - the front (margo anterior) (Fig. 47, 49), interosseous (margo interosseus) (Fig. 47, 49) and medial (margo medialis ) edges. The anterior margin at the top passes into the tuberosity of the tibia (tuberositas tibiae) (Fig. 47, 49, 54).
The distal epiphysis of the tibia has a peroneal notch on the lateral side, and the medial malleolus (malleolus medialis) directed downward on the medial side (Fig. 47, 49), covered, like the upper articular surface, with articular cartilage.
The fibula of the lower leg (fibula) is located lateral to the tibia. The articular surface of the upper epiphysis - the head of the fibula (caput fibulae) (Fig. 48, 54) - serves for articulation with the lateral condyle of the tibia. The thickened distal epiphysis ends with a lateral malleolus (malleolus lateralis) (Fig. 48, 49). The space between the diaphysis of the tibia and fibula is tightened, as in the forearm, by a strong fibrous membrane - the interosseous membrane of the lower leg, which is attached to the interosseous edges of the lower leg bones.
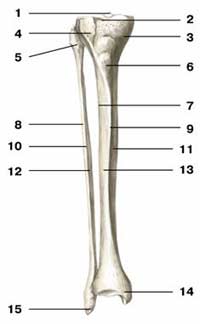
| Figure: 49. Tibia and fibula front view 1 - intercondylar eminence of the tibia; 2 - the upper articular surface of the tibia; 3 - medial condyle; 4 - lateral condyle; 5 - the head of the fibula; 6 - tuberosity of the tibia; 7 - interosseous edge of the tibia; 8 - lateral surface of the fibula; 9 - the front edge of the tibia; 10 - the front edge of the fibula; 11 - the medial surface of the tibia; 12 - interosseous edge of the fibula; 13 - lateral surface of the tibia; 14 - medial ankle; 15 - lateral ankle |
 |
The bones of the tarsus (ossa tarsi) are short, spongy. The talus connects the foot with the shin bones (Fig. 50, 51). The head of the talus (caput tali) (Fig. 50, 51) is connected to the scaphoid bone (os naviculare). The body of the talus (corpus tali) from above ends with a block of the talus (trochlea tali) (Fig. 50, 51), involved in the formation of the ankle joint. The upper and lateral surfaces of the block are covered by the articular cartilage. The lower surface of the body of the talus has articular surfaces, through which it articulates with the calcaneus (calcaneus) (Fig. 50, 51). The latter has corresponding articular surfaces on the upper surface. The anterior surface of the calcaneus, which is elongated relative to the foot in the anteroposterior direction, also has articular surfaces that serve to articulate with the cuboid bone. On the medial surface of the calcaneus body there is a process - the support of the talus. The calcaneus ends behind the tubercle of the calcaneus (tuber calcaneus) (Fig. 50, 51).
Together, the talus and calcaneus make up the proximal row of the tarsal bones. The distal row is represented by the navicular (os naviculare), cuboid (os cuboideum) and three wedge-shaped (ossa cuneiformia) bones (Fig. 50, 51).
The bones of the metatarsus (metatarsus) (Fig. 50, 51), like the metacarpal bones of the palm, are elongated and have a base, body and head. The bases of the metatarsal bone are connected to the cuboid (IV and V) and three cuneiform bones of the tarsus, while the base of the II metatarsal bone enters the gap between the forward medial and lateral cuneiform bones. The heads of the metatarsal bones are articulated with the bases of the proximal phalanges. There are five metatarsal bones in total; the first (I) is noticeably more massive.
The bones of the toes (ossa digitorum pedis) (Fig. 50, 51), or the phalanges of the fingers, also have a body, base and head. All fingers, except the first (I), have three phalanges (proximal, middle, and distal). The first toe has only two phalanges.
The lower leg, that is, a part of the lower limb of a person, consists of the following bones: tibia and fibula. Muscles are attached to these components of the human body. The fibula itself consists of a long, thin, somewhat twisted body and two widened ends. The upper end has the name - the head of the fibula, and it, due to its peculiar articular surface, is attached to the tibia. This attachment is made by an interosseous membrane. And the lower end is the ankle, which goes into the ankle joint. This is the anatomy of this part of the human lower leg.
It is thanks to the fibula that the lower leg, as well as the human foot, can rotate. But this process occurs as a result of the rotation of the two bones of the lower leg relative to each other. We owe our mobility to these bones. According to the anatomical atlas, the fibula is located in the same place as the tibia, that is, in the lower leg.
What damage is the fibula subject to?
There are several types of damage to this bone.
- Fractures.
- Cracks.
- Offsets.
With a fracture of the fibula, the integrity of the body of this element of the human body is violated. It is located in the lower leg and usually breaks along with the tibia. The causes of fractures can be: road traffic accidents, various domestic injuries, falls, blows. People involved in extreme sports are more likely to break the fibula. Also, this part of the lower leg sometimes undergoes fractures due to the lack of a balanced, full of vitamins and calcium, nutrition in elderly people.
The main types of fractures of the fibula.
- Fracture with displacement of bone particles.
- A fracture without any displacement.
- With or without fragments.
- According to the very nature of the fracture: oblique or transverse, fragmentary or spiral.
- Depending on the blow that hit the bone: direct or indirect.
Types of symptoms of fibula fracture.
- Sharp pain at the site of the injury.
- Swelling on the surface of the lower leg or even the foot.
- Clear signs of a hematoma.
- A somewhat deformed appearance of the limb itself.
- The muscles are pulled to the injury and create the effect of shortening the leg.
- Difficulty walking.
First aid for fractures of the fibula
If a bone is broken, you need to give the person a pain reliever and be sure to immobilize the leg. It is impossible to independently treat a bone fracture without medical qualifications. The victim needs to be sent to the clinic to see a doctor. To do this, you need to call an ambulance or take a person to the hospital by taxi.
Who Diagnoses Fibular Fracture?
The specialist in the treatment of fibular fractures is a traumatologist. The doctor first interviews the patient about how the injury was received. Then the doctor will require all the necessary tests and an X-ray of the lower leg. Only after a detailed study of the nature of the injuries will the doctor begin to treat the patient. After all, the fibula is treated, based on its anatomy, only by a specialist traumatologist.
How is a fibula fracture treated?
The doctor is involved in helping the patient, depending on the nature of the fracture. When a bone sticks out, sticks out, hurts badly, then these are symptoms of a serious fracture, for the treatment of which surgery is needed. If no displacement is found on the X-ray, then the patient is simply put in a plaster cast.
Surgical intervention is required when parts of the bone come off. Using special needles, the doctor will return the bones to the correct position. And metal structures will help fix the bone.
Also, a surgical operation is resorted to if the patient has an open fracture of the fibula, or if this part of the lower leg is significantly fragmented. The doctor first restores the very shape of the bone by applying broken pieces to each other. Then he holds the bone parts together with special screws or plates.
How long does it take for a fracture to heal?
There is no single period of time during which all fibular fractures are healed. Depending on the nature of the injury, as well as on the severity, on the age of the patient, on the qualifications of the attending physician, various injuries heal in different ways.
It can be argued that bone fusion will occur within two or three months. The callus itself appears after six weeks. More severe injuries are restored six months later.
How is rehabilitation after fractures going?
Four months after the fractured bone has completely healed, the rehabilitation process should begin. In time, it can drag on for six months or even more. It all depends on the severity of the fracture.
Types of rehabilitation for fractures of the fibula.
- Implementation of a scientifically developed complex of medical gymnastics, which will help to "develop" a sick leg and bring it to mobility.
- Massages performed by professional chiropractors.
- Water treatments in the swimming pools.
- Home baths for medicinal trauma.
- Self-rubbing of medicinal ointments and creams.
- A gradual increase in the load on the sore leg under the supervision of the attending physician.
In the event that the patient turned to the attending physician on time, and professional assistance was provided to him, then it will be easy to restore the leg performance. And after completing the rehabilitation course, the patient will be able to return to his usual and normal life in just six months.
- The bone may not heal properly.
- An infection can be introduced into the wound.
- The nerves or blood vessels in the lower leg can be damaged.
- Blood clots form.
- The leg is bent.
All these unpleasant moments should be corrected. And only an experienced doctor can cope with problems. In some cases, he will prescribe a second operation.
For simple fractures and small cracks without displacement of bone particles, doctors do not use radical, but more conservative treatment. It consists in immobilizing the leg with a cast or splint. A splint is applied if there is significant swelling, which prevents the application of a plaster cast on the swollen leg. Instead of a tire, a splint is sometimes used. But as soon as the edema decreases, the patient is immediately put in a cast.
Of course, the doctor carries out all these procedures only after receiving an X-ray, indicating the nature of the leg injury. In a plaster cast, a patient with simple injuries of the fibula should be about three weeks. After that, he is once again sent by the attending physician for an X-ray. Based on the results of the wound healing process, obtained with the help of an image, the doctor additionally prescribes one or another treatment for his patient.
Fracture consequences and prevention
Whatever the fracture of the fibula is, it will almost always have consequences. Even if not very complicated, sometimes insignificant. But you should always pay attention to them. And in case of detection, seek help from a qualified doctor. After all, a slight pain in the lower leg can be a signal for a more serious illness. If you ignore it, then soon all kinds of disturbances can occur in the human body, which will soon lead to serious illnesses.
And as a preventive measure, it is necessary to choose the right shoes for walking. Try not to wear high heels. When playing sports, you must use protective equipment. Do not expose your body to heavy physical exertion, which would lead to damage to the bones of the lower leg. In old age, avoid sports such as figure skating, skiing, roller skating. In winter, during icy conditions, try to use shoes with non-slip soles. Carefully behave in transport, observe traffic rules.
Other diseases of the fibula
But the fibula can be subject to various diseases. The most common is periostitis. It arises as a result of advanced varicose veins. At the initial stage, the skin of the leg is not affected by any changes. But when feeling the patient complains of unpleasant painful sensations.
The doctor begins to treat a patient with periostitis based on the testimony of an X-ray, analyzes and ultrasound scanning. The patient is prescribed medications, and he should also massage the sore leg, do rubbing. It is not recommended to treat this disease at home. The patient needs specialist care. It is better to immobilize the leg for a while.
Another disease of the fibula is osteoporosis. If you look closely at the structure of this bone, you will find that it consists of compact and spongy tissue. As a result of osteoporosis, the compact and spongy substance is destroyed. The bone becomes more hollow, and therefore brittle. Symptoms of the disease: pain in the lower leg, discomfort when walking. This disease is treated with medications that are rich in calcium and phosphorus. And as a prevention of this disease, you should eat as much milk, cheese, fish as possible.
Osteomyelitis of the fibula is also a serious disease. This is a severe purulent and infectious inflammation. Osteomyelitis affects all elements of the tibia. The cause of this disease is the penetration of dangerous microorganisms inside.
The disease develops against the background of immunodeficiency, as well as diabetes mellitus or a fracture of the fibula. This disease affects not only children, but also adults. The patient's body temperature rises sharply, the skin in the leg and knee area turns red, the person suffers from unbearable pain.
Osteomyelitis treatment is carried out only in a hospital by a professional doctor: surgeon or traumatologist. This disease is diagnosed using X-rays, analyzes and computed tomography. At home, you cannot open abscesses, because this can lead to sepsis and severe complications. In the hospital, the patient is examined by a surgeon. During the operation, the purulent focus is opened and eliminated. With medical preparations, they achieve complete recovery of the patient.
The fibula is also prone to osteosarcoma. And this disease belongs to the category of the most dangerous diseases. As a result of its development, a malignant tumor is formed in the bone. At the initial stage, the disease almost does not manifest itself. A person attributes minor pains in the lower leg to rheumatism. But he is wrong. The problem is much more serious. And after a few weeks, swelling appears, the pain becomes unbearable, and metastases develop. Treatment for osteosarcoma involves surgery to remove the tumor. After that, the patient is prescribed a course of chemotherapy.
Diagnosis of this ailment is carried out in the clinic, prescribing tests, x-rays, and bone scan to the patient. A biopsy of tissue taken from the affected area of \u200b\u200bthe fibula is performed. Previously, limbs affected by this disease were amputated. And the patients themselves did not live even five years after the operation. But now doctors have modern drugs in their arsenal. Thanks to new medicines, the percentage of patients who, even after removal of metastases, continue to live for more than five years, has significantly increased.
Osteosarcoma affects young men and women. Most often it occurs between the ages of 15-20. After fifty years, this disease is rare. The cause of the appearance of osteosarcoma can be, for example, chemotherapy, carried out as a result of another cancer. Also, the disease can intensify after a bone fracture. The impetus for its development is osteomyelitis or Paget's disease.
Diseases that affect the fibula greatly weaken it. Sometimes minor physical exertion can cause fractures, as a result of which the fibula breaks.
As a prophylaxis for diseases of the tibia, it is recommended to eat a lot of fiber and calcium. Green vegetables help to inhibit the development of pathogenic bacteria. Meat, milk, fish, cheese - these food products should constantly be on a person's table. But in order not to get sick with dangerous ailments, it is necessary to lead a correct lifestyle.
The bones of the legs play a key role in the movement and maintenance of an upright position. They carry a heavy load, so limb injuries are not uncommon. The lower legs are prone to fractures, bruises, cysts and other pathological processes. Treatment tactics are individually selected depending on their type.
Features of the structure of the tibia
Anatomical structure of the bone
The lower leg consists of two tubular bones: the peroneal, located on the outside, and the tibia, which is located medially, that is, on the inside. The anatomy of the tibia is unusual as it has a triangular shape and 3 edges:
- anterior, characterized by a pointed shape, is a lateral surface;
- medial, or collateral (located on the side), which, due to protrusion forward, is easily felt through the skin;
- the interosseous edge, which faces the fibula.
The tibia consists of 3 sections:
- proximal pineal gland;
- distal pineal gland;
- body connecting two pineal glands.
The proximal epiphysis of the tibia is represented by the lateral and medial condyles. These structures connect the tibia and femur. Outwardly, the condyles look like protrusions that are located at the top of the bone. The metaphysis is located in the proximal part, that is, the thickened edge that surrounds the surfaces of the joints.
On the surface of the upper epiphyseal zone there is an intercondylar tubercle (mound): from the side - internal, from the front - external. The shape of the distal pineal gland is rectangular. In its upper part there is a peroneal notch. The ankle groove is located behind.
Damage classification

Fracture of the tibia
Possible causes of injury to the bones that make up the lower leg:
- road traffic accidents:
- jump from a great height;
- a strong turn of the lower limb, in which the foot was fixed, for example, while skiing (often a child suffers from such an injury);
- falling on the kneecap (for example, if you run quickly and stumble);
- twisting of the lower limb in the ankle joint;
- hit with a blunt object.
Damage classification:
- bruises;
- cracks;
- fracture;
- epiphyseolysis: destruction of the growth zone of the bone structure.
Fractures are divided into:
- transverse, in which the damage is perpendicular to the axis of the bone;
- oblique: violation of the structure at an angle;
- helical, where the break line looks like a spiral;
- shrapnel, when a bone breaks into 3 or more fragments;
- intra-articular, in which the medial ankle and condyles are injured.
In addition, fractures can be open or closed. When opened, soft tissues are damaged, wound and bleeding are formed. With a closed, for example, fracture of the upper proximal tibia, the fragments do not tear the tissue and do not come out.
Fractures are more susceptible to the ankle zones (the bone of the distal tibia), the condyle, the posterior and anterior tibia.
Symptoms and confirmation of the diagnosis

X-ray to check for ankle fracture
Any type of fracture is characterized by certain features:
- sharp pain both at rest and when trying to stand on the lower limb. It is also caused by pressing the heel;
- deformity of the lower leg, noticeable on external examination;
- crackle at the slightest movement;
- the leg cannot be bent, lean on it;
- increasing tissue edema, the gradual appearance of bruising;
- with an open fracture, a bleeding wound.
To clarify the diagnosis, the doctor prescribes an x-ray. The picture will help determine the severity of the injury and choose the tactics of treatment.
With an intra-articular fracture, arthroscopy is performed to check the condition of the intra-articular ligaments. If nerve fibers are involved in the pathological process, electroneuromyography is performed. The specialist may consider it appropriate to appoint an MRI or CT scan.
Treatment

Pain medications
In case of a fracture of the shin bones, first aid should be provided to the victim as soon as possible.
- Limb immobilization. The splint can be made from any means at hand.
- Application of a tourniquet. Required for severe arterial bleeding. If a vein is damaged, a tourniquet is applied below the wound. If the artery - the blood from it is bright red and comes in jerks - the tourniquet is applied above the wound.
- Removal of large foreign bodies around the damaged area, applying a sterile dressing. Will prevent infection.
- Taking an anesthetic.
Then the victim must be taken to the hospital, where he will be given an accurate diagnosis and appropriate treatment. It can be conservative or operational.
If there is no displacement, immobilization with a plaster cast is sufficient.
It is impossible to remove the cast without the doctor's permission, it is fraught with the displacement of parts of the broken bone and the development of complications.
Skeletal traction is most often required. A special needle is passed through the calcaneus, and the limb itself is placed on the splint. A load is suspended from the spoke, the weight of which is determined by the individual characteristics of the victim: body weight, the state of the muscular apparatus, the nature of the injury.
Duration of traction - up to one month. If a callus formation is detected on the X-ray, a plaster cast is applied to the limb.
You need to wear it for 10 weeks.
Surgical intervention is required for complex fractures when conservative methods of therapy are ineffective. Usually, within a week, the patient is monitored in a hospital, conducting a comprehensive examination.
For surgical intervention, various metal structures are used, which allow for the procedure of osteosynthesis. On average, bone fusion occurs within a month.
Features of the rehabilitation period

Massage to improve blood circulation in damaged tissues
To restore blood circulation and muscle tone, after removing the plaster, appoint:
- massage;
- a course of special gymnastic exercises;
- physiotherapy.
Thanks to massage, blood circulation in damaged tissues is improved, they regenerate faster.
They help to speed up the restoration of functions of the damaged leg. The first workouts bring a lot of unpleasant sensations, you have to be patient and endure pain.
Physiotherapy is prescribed taking into account the nature of the trauma suffered:
- electrophoresis. Medicines enter deep into the tissue through the action of an electric current;
- magnetotherapy. Improves blood circulation, accelerates tissue regeneration;
- ultrasound. Improves the penetration of painkillers into damaged tissues;
- diode dynamics. Accelerates regeneration through exposure to alternating currents.
If the victim is prescribed an operation with the installation of metal structures, physiotherapy is stopped. In this case, ultraviolet radiation is indicated, which promotes the production of vitamin D (necessary for the absorption of calcium).
Bone cyst formation

Aneurysmal cyst
If the tibia hurts when walking, in some cases this may indicate the development of a bone cyst. With this disease, a thickening forms in the bone cavity.
The cause of the pathology has not yet been identified, but it is known that circulatory failure can provoke the development of the disease. As a result, the movement of biological fluid inside the bone is disrupted and lysosomal enzymes are activated, which provoke the breakdown of collagen, glucosaminoglycans and protein compounds. According to the classification of diseases of the ICD 10, a bone cyst is a tumor-like formation. She was assigned the code M85.4.







")
- Million people Multiples and submultiples
- Mesentery of the large intestine and its relationship with neighboring organs Common mesentery of the small and large intestine
- Toddler Baked Potatoes
- Potatoes in the oven for a baby 1 year old
- Human chest anatomy
- Than to consider gossips to work, it is not better for yourself, godfather, to turn
- Why are you shy and why do you need it?
- Sour cream with cookie dough
- How to make an omelette for a child: a step-by-step recipe Steam omelette for a child 1 year old recipe
- What happens if you don't eat for a long time?
- How to cook a vegetable salad for a child: simple recipes
- Folic acid dosage: learning to take it right!
- How many liters of water should you drink per day?
- All Quests, tasks for the game, brownies!
- The body can synthesize glucose
- Lose weight without harm to health after 55 years
- Womanizer behavior men psychology
- Anatomy and possible damage to the tibia and fibula
- Skeleton of the free part of the lower limb
- Hernioplasty of an umbilical hernia: types, possible contraindications, preparation for surgery, recovery period, reviews